
AUSTRALIA is one of the worst performing wealthy countries in terms of vaccinating the population against COVID-19, with 28.27% of the population fully vaccinated (2 September 2021). This is due to a number of factors, including an inadequate supply, age-based eligibility barriers, and hesitancy among certain groups of the population to receive the vaccine.
Medical experts had earlier stated that for all those over 12 years of age, at least 80% will need to be fully vaccinated if we are to achieve herd immunity, the level required to get the virus under control (here, and here). The level of COVID-19 vaccine coverage that countries should aim for has been an intense focus of public health researchers throughout the pandemic. While estimates vary, it is clear that Australia will need very high vaccination levels to avoid large outbreaks and substantial losses of life (here). The recent Doherty Institute modelling report estimates that at even very high levels of vaccine uptake (80% of people aged 16 years and over), additional social measures would likely be required to constrain epidemic growth.
National Cabinet has set a series of targets to move the country through four phases of recovery from COVID-19. The phases are suppression (where we are currently), transition, consolidation, and the final phase. In order to move to the transition phase 70% of eligible Australians will need to be fully vaccinated. To move into the consolidation phase, 80% will need to be fully vaccinated.
There may be few easy “nudges” to sway people to get vaccinated as soon as possible in order to reach National Cabinet targets. We know that offering financial incentives can be an effective method (here, and here) to change health-related behaviours in other situations, including to improve the uptake of preventive health interventions.
In June 2021, the Taking the Pulse of the Nation survey from the Melbourne Institute asked Australians about their willingness to get vaccinated.
Based on their initial responses, people were categorised into three groups (Table 1) of decreasing degrees of commitment to the vaccination.
Table 1: Categorisation of respondents and offer of hypothetical cash incentive
| Categories of respondents | Responses | Hypothetical cash incentive offered |
| I. Committed to immediate vaccination | 1) Already had at least one dose of the vaccine.
2) In principle willing to have a vaccine, as soon as possible. |
No |
| II. Committed to vaccination, but not immediately | In principle willing to have a vaccine, 1) but currently prefer to wait;
2) but unsure when. |
Yes |
| III. Uncommitted to vaccination | 1) Unsure of whether to have a vaccine at all.
2) Not willing to have a vaccine. |
Yes |
Hypothetical cash amounts of $25, $50 and $100 were randomly offered to respondents categorised as “II. Committed to vaccination, but not immediately” or “III. Uncommitted to vaccination” to see if it would change their intention to “vaccinate immediately”.
From the original full sample of 2400 respondents (representative of all Australian residents 18 years and over), we analysed the 1101 respondents 50 years of age and over, as only they were eligible for voluntary vaccination during the full survey period (31 May – 18 June 2021).
Figure 1: Willingness to get vaccinated
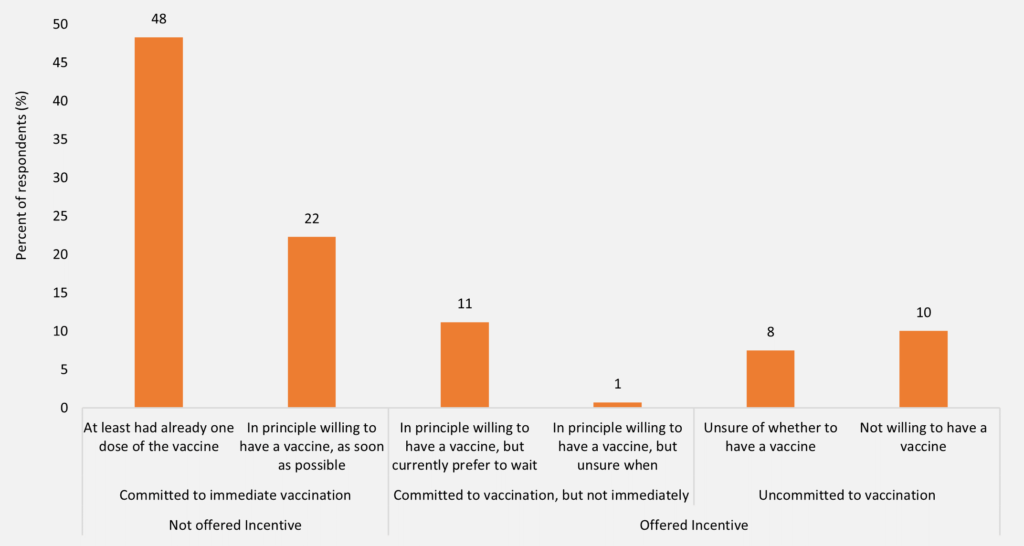
Source: Data from the Taking the Pulse of the Nation survey, representative of the Australian population aged 18 years and over. This study uses only those 50 years and older (n = 1101). The vertical axis indicates the proportions (%) based on weighted responses. Survey question: (1) “Are you willing to have the COVID-19 vaccine?” – Yes/No/Don’t know/I have had it already and (2) “If yes, “When would you like to be vaccinated?” – As soon as I am eligible (or is possible)/willing to wait/don’t know.
KEY INSIGHTS
1. Seven out of 10 Australian residents 50 years and over were committed to immediate vaccination.
Figure 1 (above) shows that 70% of respondents 50 years and over were committed to immediate vaccination – 48% had at least one vaccination and 22% were committed to having their vaccination as soon as possible. However, 12% were committed to getting the vaccination, but not immediately. The remaining 18% were uncommitted to being vaccinated – with 8% unsure and 10% unwilling. The COVID-19 vaccinations currently available in Australia require two doses per person of the designated vaccine to provide the fullest coverage from the virus.
2. Offering cash incentives can help hasten the vaccination roll-out, but only for men and only for payments of at least $100
We examined the group we call “II. Committed to vaccination, but not immediately” (Table 1). To assess the extent to which these preferences might be altered through incentives, we asked these respondents if they would like to be vaccinated as soon as possible, should they be offered a hypothetical cash incentive. Hypothetical cash amounts of $25, $50 and $100 were randomly offered to these respondents. We found that men were more willing to change their intention to get vaccinated immediately in response to any sort of cash incentive (43% men versus 20% women), and even more so as the payment increases (61% versus around 18% for $100) (Figure 2).
Figure 2: People (aged 50 years and older) who would get vaccinated sooner if offered cash incentive
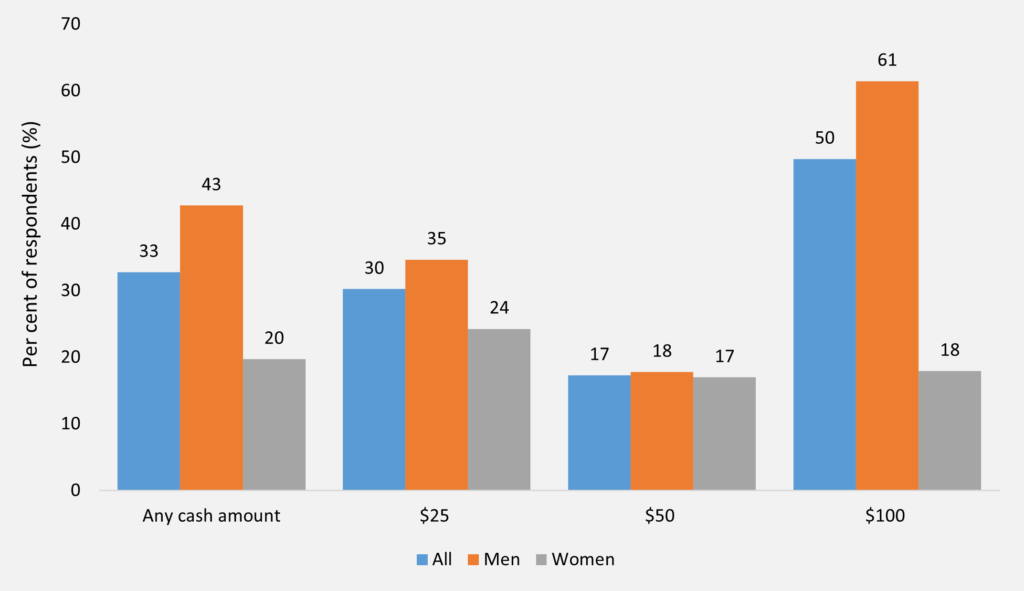
Source: Data from the Taking the Pulse of the Nation survey, representative of the Australian population aged 18 years and over. This study uses only those 50 years and older (n = 1101). This figure depicts the responses of those who are committed to vaccination but not immediately (n = 131). The vertical axis indicates the proportions (per cent) based on weighted responses. Those committed to vaccination but not immediately were asked if they would like to be vaccinated as soon as possible if they were offered a cash incentive. Hypothetical cash amounts of $25, $50 and $100 were randomly offered to respondents and their responses were recorded as “Yes”, “No” or “Don’t know”.
3. Offering cash incentives is unlikely to increase the rate of vaccination among the uncommitted Australian population
We lastly examined the group we call “III. Uncommitted to vaccination” (Table 1). We further questioned the 18% of respondents most hesitant towards vaccination and asked whether they might change their minds if they were offered a cash incentive to be vaccinated as soon as possible. Hypothetical cash amounts of $25, $50 and $100 were randomly offered to these respondents. We found that the rate of vaccine hesitancy was decidedly higher among this group, as 96% of respondents continued to say “No” or “Don’t know” in relation to getting the vaccine as soon as possible, for any level of a cash incentive (Figure 3). This suggests that offering cash incentives alone is unlikely to sufficiently increase the rate of vaccination in the Australian population. In other analyses, we found that for the under 50s who are uncommitted to vaccination, no more than 16% say that they can be budged by an incentive such as a cash payment of the same size.
Figure 3: People (aged 50 years and older) uncommitted to vaccination, but would change their mind if offered cash incentives
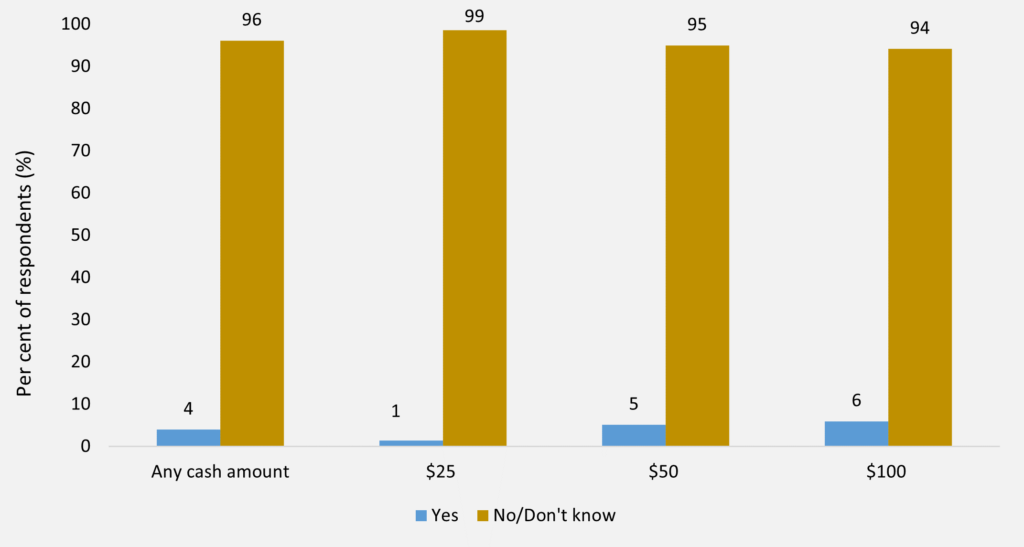
Source: Data from the Taking the Pulse of the Nation survey, representative of the Australian population aged 18 years and over. This study uses only those 50 years and older (n = 1101). This figure depicts the responses of those who are uncommitted to vaccination (n = 193). The vertical axis indicates the proportions (%) based on weighted responses. Those uncommitted to vaccination were asked if they would like to be vaccinated as soon as possible if they were offered a cash incentive. Hypothetical cash amounts of $25, $50 and $100 were randomly offered to respondents and their responses were recorded as “Yes”, “No” or “Don’t know”.
Future directions
For some people, no amount of cash incentive is going to make them change their mind if they are opposed to getting the vaccine. As a last resort, this may imply some level of legislated compliance enforcement is required to reach the national cabinet targets of 70% vaccination rates to leave lockdown and an 80% rate to relax border restrictions and other measures.
In the survey over the period 31 May – 18 June 2021, we found that 70% of the adult resident population in Australia aged 50 years and over had already received at least one dose of the COVID-19 vaccine or was willing to receive it immediately. In the meantime, the number of vaccinations in the main affected states has increased substantially, given the wave of infections currently hitting NSW and Victoria in August 2021.
For those hesitant to receive the vaccination, through incentives of amounts between $25 and $100, an additional 5% could be convinced to get the vaccination immediately. Altogether this is already less than the 80% of the 50 years and over population, who have got or would get a vaccination immediately, to reach National Cabinet target levels of vaccination. In addition, all those aged between 12 and 49 years would also have to reach the same target levels of full (two-dose) high-efficacy vaccination.
Without complete voluntary compliance from all people 12 years old and above, other measures should be considered to reach those who are uncommitted and steadfastly hesitant towards getting the vaccine. Policymakers may be forced to resort to more “sticks” (legislated compliance enforcement), in addition to “carrots” (voluntary incentive payments) to achieve the national cabinet targets, including mandated vaccine requirements for day care, aged care, school enrolment, public transport and mass public event attendance to name a few examples. One option is a vaccine passport to normality — allowing those that have been vaccinated to enjoy everyday activities such as dining in a restaurant, attending a concert, or travelling. The Europeans have done this with the EU Digital COVID Certificate, which provides proof the holder has been vaccinated, tested negative to SARS-CoV-2, or had been infected in the past and recovered.
The consequence of not achieving at least National Cabinet target vaccination rates would be long term medical, social and economic disruption of the country. High levels of avoidable morbidity and mortality would likely be coupled with repeated cycles of outbreak, lockdown, temporary recovery, and further outbreak. Assuming that supplies are available and accessible for everyone, if all of those who medically can receive the vaccine altruistically did so, Australia would very soon be hitting the targets needed to “live with” COVID-19.
Further information
Datasets: This analysis uses data from the Taking the Pulse of the Nation survey – the Melbourne Institute’s survey of the impact of COVID-19. The aim of the fortnightly survey is to track changes in the economic and social wellbeing of Australians living through the effects of the coronavirus pandemic while adapting to various changes in federal and state government policies. The survey contains responses from 1200 people aged 18 years and over. The sample is stratified by gender, age and location to be representative of the Australian population. The current analysis draws on survey responses collected from wave 34 and wave 35 over 31 May – 18 June 2021.
Professor Dr John P de New is Professorial Fellow and Program Coordinator at the Melbourne Institute: Applied Economic and Social Research, University of Melbourne.
Dr Kushneel Prakash is a Research Fellow at the Melbourne Institute: Applied Economic and Social Research, University of Melbourne.
The statements or opinions expressed in this article reflect the views of the authors and do not represent the official policy of the AMA, the MJA or InSight+ unless so stated.
“…legislated compliance enforcement…”
So innocently dropped in the sentence.
I thought medicos were familiar with the concept of consent?
You do know that what people say they will do , and why, and that they actually do, and why, are not the same? Right?