
“WHAT should I do?” asks the expectant mother going through labour. “Nothing dear,” says the doctor. “You’re not qualified.”
While that might be a scene from Monty Python’s The Meaning of Life (1983), it is fair to say that until recently consumers have played a minor role in their own health care. They are increasingly moving to centre stage; however, the research sphere must foster more growth in co-developing strategy and direction, with the consumer at the centre.
People with multiple sclerosis (MS) have always been a key pillar for MS Australia, with people affected by MS represented at every level within the organisation. In 2001, MS Australia set up the Australian MS Longitudinal Study that has been collecting patient reported outcomes for the past 20 years. The evidence generated from these lived experiences has been used to effect change for those with MS, their families, and carers, including using patient reported outcomes as a measure of disease progression, linking modifiable lifestyle factors with health outcomes for people with MS, and successfully advocating for subsidies for air conditioning to combat heat fatigue.
In addition to driving forward data-informed medical and support services, we have been extending the influence of patient voice in our research strategy. To this end, we recently repeated our Research Priorities survey, which was first carried out in 2016.
The latest edition of the survey carried out in 2021 involved 3000 respondents, of whom 1541 were people with MS. This was a marked increase from 772 people with MS in 2016.
Responses were collected anonymously, and various demographic questions were asked to help understand how representative the study sample was of the Australian MS community. The survey was answered by the equivalent of one in every 16 Australians living with MS, and all types of MS were represented: 990 respondents were people with relapsing remitting MS (the most common form), 284 were people with secondary progressive MS, 128 had primary progressive MS, and the remaining 130 either were not sure of what type of MS they had or they reported having some other variant. Overall, our analysis showed that the characteristics of the survey respondents were very similar to the wider Australian MS population in terms of age, sex, disease type and disease severity, enabling us to confidently use the survey findings to inform our strategic direction and our research strategy going forward. The survey was also taken by family members of those with MS, carers and professionals involved in the MS community.
“Finding a cure” was the top priority for our survey respondents. This was consistently the top priority despite MS status, type of MS, severity of MS or duration of the disease. The second priority was “preventing MS”, followed very closely by “better treating MS”.
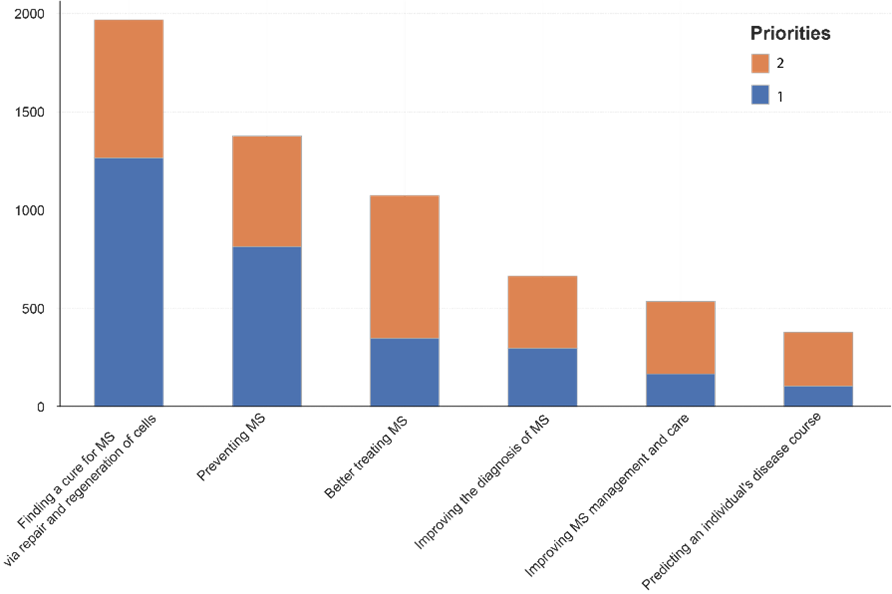
Figure 1: The top priorities of the survey participants. 3000 members of the Australian MS community that took part in the survey ranked the areas of priority from 1 to 6 (with 1 being the highest ranking and 6 being the lowest); the top 2 rankings are displayed here.
The top priority is unchanged since 2016. However, “preventing MS” has increased in importance since 2016, bumping “better treating of MS” into third place. One possibility to explain this change might be that given the rapidly advancing battery of treatments available for the most common form of MS (relapsing remitting MS), people have altered their priorities around prevention and treatments. Over the past 15 years, there has been a tripling in the number of treatments for relapsing remitting MS. These medications are having a large impact on the lives of people with MS, with disability milestones being delayed and the number of relapses reduced. However, this difference might just be due to chance, and further analysis would need to be carried to confirm this.
Other priorities included “improving the diagnosis of MS”, “improving MS management and care”, and “predicting an individual’s disease course”. Respondents also replied to several questions relating to research priorities and more granular questions designed to tease out further details, and to validate initial high level questions.
One area of particular interest was symptoms, including which symptoms people with MS thought required more emphasis. Here, different groups had slightly different priorities, but there were common themes. The top six symptoms across the respondents with different MS types and severity were cognitive function, walking and mobility, balance and falls, fatigue, pain, and vision problems.
We also asked about areas of importance when it came to advocacy. There were 11 areas of advocacy assessed, including improving access to neurologists, MS nurses and telehealth. Open text fields were also included to ensure that every aspect of MS research and advocacy was covered. The top area for advocacy among respondents was additional funding for MS research, followed by approval of new MS medications and meeting the needs of those not eligible for the NDIS.
It is outstanding that a substantial number of people with MS or a connection to MS were able to complete the survey, which has provided much insight into what needs to be addressed. These data will be used to navigate MS Australia’s direction for research and advocacy, but as the saying goes, data are only the raw material of knowledge, and it is the application of the data that results in knowledge and better consumer-centric direction.
Hamish Campbell, Julia Morahan, Rohan Greenland, Desmond Graham are members of the MS Australia Board and management team. Associate Professor Graham is the chair of the MS Australia Board and lives with MS, Rohan Greenland is the CEO, Doctors Morahan and Campbell are the Head and Deputy Head of Research at MS Australia.
The statements or opinions expressed in this article reflect the views of the authors and do not represent the official policy of the AMA, the MJA or InSight+ unless so stated.
Dear Benjamin
Thank you for your comment, trigeminal neuralgia is both a significant and very painful MS symptom. As you have probably noted, pain does rank quite highly in the priority list of symptoms (pain of course includes trigeminal neuralgia). Pain in MS is poorly understood, and even prior to this survey, pain was an area of interest for us. We have held pain workshops where we gathered pain specialists, neurologists, MS nurses, and other healthcare professionals to try and increase understanding in this area, as we appreciate there is still a lot of work to do in this area moving forward. We will continue to advocate about this so that people living with MS and TN will not feel alone, as you have experienced.
While the first three choices to be no Brainers, I believe the fourth should be finding a cure for the ms sufferers with trigeminal neuralgia. The fourth and fifth, better treatment and prevention of trigeminal neuralgia but the sixth and seventh should be better education of ms and trigeminal neuralgia in hospital’s. Given trigeminal neuralgia to be one of the most painful ailments known to medical science, I’m shocked at how little hospital staff know about either ailments. After having been admitted to hospital several times for TN I felt truly alone being asked time and time again by doctors and nurses “What is MS/TN, you’ll haft to run me through it.”. to only then receive semi adequate care, treatment and understanding.