From 1 December 2015, Laureate Professor Nicholas Talley has assumed the role of Editor-in-Chief at the Medical Journal of Australia.
As one close reader of the MJA, I cannot imagine anyone in Australia better qualified than Professor Talley to head what I choose to believe is the leading medical journal in the southern hemisphere. Professor Talley’s many affiliations will, I am sure, strengthen the Journal in arenas national and international. I congratulate him on his appointment and wish him, together with all Journal staff, the best of fortune for coming years.
It has been a great privilege to serve the Journal over recent months. I thank all staff at the Journal for advice and assistance. The Board of the Australasian Medical Publishing Company, chaired by Mr Richard Allely, and the President of the Australian Medical Association, Professor Brian Owler, have also provided unqualified support, so I thank them too. As a consulting editor, Professor Jeffrey Zajac has also contributed during the interval between Editors-in-Chief.
As a refereed journal, our warmest gratitude to our dedicated reviewers: they are listed here.
I am grateful for the experience of editing the MJA: there is plenty to learn.
My best wishes to all readers of the MJA. The future looks bright indeed.
The Medical Journal of Australia is without doubt the most important general medical journal in Australia, with a history dating back over 100 years. It is therefore a great honour and privilege to commence as your new Editor-in-Chief.
My professional interests span clinical practice, medical education and research, medical leadership, health policy and social justice. My goals as editor are to build on the outstanding DNA of the Journal, further increasing its relevance and readability, and attracting the highest quality submissions. We will aim to build on the Journal’s rich heritage by continuing our practice of publishing the best clinical science papers that have the potential to transform practice, including clinical trials and comparative effectiveness research. We will also aim to inform readers on advances in medical education, and cover issues from medical leadership to re-engineering our health system. We will continue to seek expert reviews, editorials and commentaries, meta-analyses and guidelines, and the latest news and information that everyone in practice needs to know. It is my goal to reinforce the unique role that the Journal plays as the pre-eminent publisher of Australian medical research and as a vital platform for translating research into practice, as well as helping to inform the broader health policy debate. This is part of the Journal’s success and why it is relevant to clinicians, researchers and academics across the nation.
The MJA is prestigious and influential, but another advantage to publishing with us is that much of the content including our research content is published freely on our website at mja.com.au, without the waiting period often imposed by other journals. I can also assure readers that as Editor-in-Chief, I have a guarantee of editorial independence and I will fiercely guard this independence on your behalf. For the nearly 32 000 subscribers who receive the MJA in print, and the many others who read the Journal online, the team will work tirelessly to provide the best medical journal experience possible.
We live in a world that, in terms of connectivity through social media, is rapidly shrinking, and the MJA has an important role to play not just nationally but globally. We will therefore now be encouraging locally relevant international articles. And we will continue to tackle in our pages articles that highlight the tough health issues we all face and provide possible solutions, from the health needs of Indigenous Australians to the health impacts of global migration, population growth, dwindling resources, an ageing population and climate change, to name a few. We will look both out to the world and across Australia to find the objective data that can help guide us all. We will seek balance among the many expert opinions and will aim at all times to be rigorous, evidence-based and transparent.
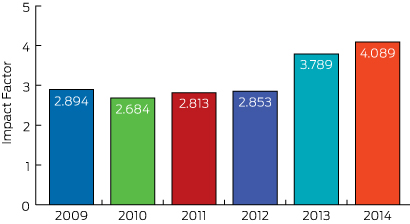
Whether any of us like it or not, our performance in medicine is being increasingly measured and critiqued, and it’s no different for medical journals. Clinicians and academics want to publish in the best medical journals and one metric applied universally is the impact factor, calculated by counting the mean number of citations received per article published during the previous 2 years. In the best journals, editors arguably “live and die” by the journal impact factor published each year. The impact factor is flawed (some argue fatally so) and is not used by the National Health and Medical Research Council; but it can’t be ignored either!1,2 In 2015, the MJA, your national journal, ranks in the top 20 general medical journals worldwide and has a highly respectable impact factor of 4.089 (Box, previous page). I am pleased to say that the impact factor of the MJA has risen and I anticipate over the coming years that it will continue to rise (as will other metrics of excellence) as we further increase the quality and reach of what we publish.
We welcome your best work being submitted for consideration. Our acceptance rate is currently falling (as marks all of the best medical journals) but I can pledge that your medical articles will be expertly peer reviewed and edited before publication. The editorial team will do its utmost to ensure it makes the best possible decisions, and we will work hard with authors to help them publish polished, excellent contributions.
Finally I would like to acknowledge and thank Professor Charles Guest in his capacity as Interim Editor-in-Chief for his stewardship of the Journal in the second half of 2015. He has been instrumental in supporting our editors and maintaining the continuity and the quality of the Journal.
Thank you for reading the MJA. You can expect that the Journal will be further increasing its scientific reputation and international presence over the next few years, and I hope you will be part of it if you have a contribution you wish to make. We welcome suggestions and feedback so we can further improve the Journal on your behalf. I am committed to strengthening your clinical practice through its pages and look forward to our journey together.
A summit of experts from around the world is meeting in Washington to consider the scientific, ethical and governance issues linked to research into gene editing. Convened in response to recent advances in the field, the summit includes experts from the US National Academy of Science, the UK’s Royal Society and the Chinese Academy of Science.
Gene editing is a new technique that allows one to change chosen genes at will. It has been applied to many organisms but a recent report from China showing the modification of human embryos using a technology known as CRISPR/Cas9 mediated editing set alarm bells ringing.
Here’s the main fear: if you modify an embryo (and therefore also its germline), you change not only the person that embryo will become but also its future sons, daughters, grandsons and granddaughters.
Since we don’t know much about this technology, it’s right to stop and think about it. But personally I’m not overly concerned: we’ve been here – or somewhere quite like it – before.
Learning from history
In 1975, scientists met at Asilomar on the Californian coast to discuss a moratorium on recombinant DNA (that’s DNA formed from combining constituents from different organisms).
Alarm bells had started ringing when scientists realised they could combine the DNA from a monkey virus with a circle of DNA called a plasmid, carrying an antibiotic resistance gene purified from the human gut bacteria, Escherichia coli (E. coli).
This cocktail sounded dangerous and scientists discussed a voluntary moratorium on certain experiments, as well as sensible guidelines for containing recombinant material within laboratories.
Horizontal gene transfer occurs in nature when DNA is carried between species by viruses and related carriers. Jer Thorp/Flickr, CC BY
Regulations and guidelines are still in place and after 40 years few, if anyone, has been harmed by recombinant DNA. And there have been no reported outbreaks of recombinant material that have significantly affected human health or the environment.
All technologies, including different agricultural practices, have upsides and downsides, and most medicines and treatments have side effects. But recombinant DNA would now have to be classed among the least dangerous of scientific developments.
Understanding science
One reason the technology has proven so safe may be that genetic recombination has been going on for millions of years. In most cases, genes are simply passed on from parent to child. But horizontal gene transfer also occurs in nature when DNA is carried between organisms or even species by viruses.
Over time, DNA is naturally swapped around and moved. Though you may have eaten transgenic plant products, I very much doubt you’ve noticed.
There was a fear “mad scientists” would invent dangerous new superbugs and killer viruses. Perhaps this could have happened, but sadly there are enough pre-existing dangerous substances and naturally occurring diseases, which have been perfected by evolution, out there already. So germ warfare scientists are more likely to just use them.
Another fear was that researchers would modify humans. Most countries quickly outlawed the modification of human germ cells and, to my knowledge, it has never occurred. In general, scientists seem to have obeyed the regulations.
But another reason is that it has proved difficult to introduce new genes into mammalian cells. It’s legal to modify human cells, such as blood stem cells, to cure genetic diseases. But human cells are among the hardest to modify. Human “anti-viral” software seems so powerful that it inhibits the stable insertion and expression of new DNA.
The promise of gene editing
I’m sure you’ve met people who’ve had their teeth straightened or undergone cosmetic surgery. But you’ve probably never met anyone who’s had gene therapy or ever seen a transgenic animal.
Could that change with gene editing? Gene editing is so precise that one doesn’t just lob in a new gene and hope it works; what one does is edit the existing gene to eliminate any misspellings, introduce beneficial natural variants, or perhaps cut out or insert new genes into chosen locations.
Our anti-viral software may not even detect what’s happened. And provided there aren’t any “off-target’” effects, where we hit the wrong gene, there may be no or minimal side effects.
Now that it’s so easy to meddle in human genes, why shouldn’t we worry?
The new technology is a game-changer – but it’s not a runaway phenomenon, like releasing cane toads, blackberries or rabbits into Australia. After 40 years, there have been few, if any problems, with genetically modified organisms. And the experiments – though much easier now – are still so elaborate and expensive that the technology will spread slowly.
We’ll likely remain cautious about modifying human embryos and about any modification that may be passed on to the next generation. To date, consent is required for all treatments. And while patients may opt for experimental cancer therapy or surgery, we always try to think carefully when others, who cannot consent, will be affected.
Some people will even ask why it’s wrong to correct a defect that could haunt future generations. Or, if we could introduce a gene variant that protects people from cancer – such as creating a duplication of the tumour suppressor gene p53 – why wouldn’t we want that for our children?
Genetics is a branch of science that’s ripe for discussions, and conversations on recombinant DNA, gene therapy, cloning and stem cells have all gone well. Guidelines have been sensible and researchers have largely complied with them.
The very fact that people from across the world are gathering to discuss the issues surrounding the latest breakthroughs in gene technology is a very strong sign that the science will be used responsibly. One hopes that the concurrent meeting on climate change in Paris is also a victory for science.
The nation’s largest health insurer will no longer cover the costs of many patients who become sick or injured in hospital as a result of what it deems to be avoidable medical complications or errors under the terms of a deal struck with major private hospital operator Healthscope.
In an important development for Medibank Private as it tries to squeeze down on payouts, the insurer and Healthscope have reached agreement on a two-year contract that includes provisions regarding the safety and quality of care.
While the details of the arrangement have not been publicly disclosed, it is believed to include clauses regarding liability for costs arising from hospital acquired complications and avoidable readmissions.
The deal follows an attempt by Medibank earlier this year to pressure Calvary Health Group into accepting responsibility for 165 complications the insurer described as preventable, including deep vein thrombosis and maternal death arising from amniotic fluid embolism.
The demand initially led to a breakdown in negotiations, but eventually Medibank and Calvary reached agreement – though the terms remain confidential.
A senior hospital executive has warned the issue could become a “flashpoint” for the sector.
“To use quality and safety to some extent as a Trojan horse, and taking the role of arbiter of quality and safety for the contributor is interesting,” Calvary Chief Executive Mark Doran told a UBS Australasia conference in Sydney in November. “It means you’re in conflict with the medical profession, who see themselves as the arbiter of quality and safety for their patient. If you don’t engage with them, you risk them pulling back.”
Medibank’s deal with Healthscope is significant for the insurer because the company operates 46 private hospitals across the country and provides around 165,000 episodes of care to Medibank members each year.
Healthscope Chief Executive Officer Robert Cooke insisted his company was “working in partnership” with Medibank in reducing waste and inefficiency.
“Healthscope has a longstanding commitment to improving our patients’ experience in hospital, including robust safety and quality programs,” Mr Cooke said. “Medibank’s focus on reducing hospital acquired complications and avoidable readmissions is complementary to the quality data we have been publishing since 2012.”
Outgoing Medibank Managing Director George Savvides said the Healthscope deal was one of a number of “performance-based contracts” it was seeking to strike with hospital providers, and set an example of how insurers and providers could work together to “maintain excellence…while also reducing rising health costs”.
But AMA President Professor Brian Owler said “close attention” needed to be paid to what Medibank was trying to do.
Professor Owler said that because hospital expenses and prosthetics together made up about 85 per cent of private health fund costs, it “stands to reason” these would be a focus for Medibank.
The major health funds have commissioned a report on prosthetic costs amid complaints they are paying $800 million a year more on devices compared with the public sector.
But Professor Owler warned that the insurer should not pursue cost-cutting under the guise of patient safety and quality assurance.
“What we don’t want is punitive measures that punish patients and interfere in what would otherwise be routine clinical cases in order to save money,” the AMA President said.
While some serious mistakes, such as operating on the wrong limb or transfusing the wrong blood type, should never occur, Professor Owler said complications were an unfortunate but inevitable part of clinical practice, particularly when doing high-risk procedures on patients with multiple co-morbidities.
“Of course, every effort should be made to minimise these complications, but we are never going to be able to eliminate them,” he said.
Professor Owler said if Medibank’s true goal was to increase patient safety and improve quality, imposing financial penalties was the wrong way to go about it.
He said there was already a multilayered system in place to improve quality of care, including clinical groups, peer reviews, continuous professional education and training and accreditation standards.
“Financial penalties should not be the major lever to try and improve the quality of care,” Professor Owler said. “Doctors and nurses are already very motivated to improve the outcomes of care for their patients.”
A woman in Germany who was blind for 17 years has regained her sight, in all but two of her multiple personalities.
The woman, ‘B.T’ suffered an accident in her younger years and gradually lost her vision. According to a study in PsyCh journal, at the time, doctors diagnosed her with cortical blindness from the trauma of the accident.
Years later, she visited Munich psychotherapist Dr Bruno Waldvogel to help with her dissociative identity disorder. Previously referred to as multiple personality disorder, it causes sufferers to have two or more distinct personality types or states. The main cause is severe and repeated trauma in childhood, often before the age of 5.
Dr Waldvogel noted that B.T experienced over 10 different personalities of varying ages, genders, temperaments and other personality traits. Some spoke German, others English and others a mixture of both as she had spent time in her childhood in an English-speaking country.
After four years of psychotherapy, she started seeing letters on a page while she was in one of her adolescent male states. In time, all but two of her personalities were able to regain sight.
An EEG test proved that B.T wasn’t lying about her disability. In one of her two blind states, her brain showed it wasn’t responding to the visual stimuli that sighted people would respond to, despite her looking straight at it.
When she was tested with her sighted personality, her response was normal and stable. They noted in the study that “a switch between these states could happen within seconds”.
Researchers believe that the loss of the woman’s vision was actually of a psychogenic nature and that the two blind personality states are possibly for retreat.
Research author Dr. Hans Strasburger of Ludwig Maximilian University said in an article in Braindecoder: “In situations that are particularly emotionally intense, the patient occasionally feels the wish to become blind, and thus not ‘need to see.'”
B.T.’s case shows that “differences between personality states are not limited to higher-level processing but can differ with respect to the fundamental processing of early sensory information and corresponding perceptual change,” they said. “It therefore provides compelling evidence for the existence of the dissociated identities in a more biological sense.”
A new community-led campaign hopes to build awareness among Australians about the importance of the Medical Research Future Fund.
The television and online campaign features Carrie Bickmore, Ita Buttrose, Natasha Stott Despoja, and former Australians of the Year Sir Gustav Nossal and Professor Patrick McGorry.
It will ask “What’s the fuss?” about medical conditions such as dementia, brain cancer, heart disease, and mental illness.
Medical Research Future Fund (MRFF) Action Group Chair Peter Scott says: “The MRFF is the serious investment in health and medical research that Australia needs, and we are grateful that it is receiving the fuss it deserves thanks to so many high profile people being so generous with their time in filming with us, simply because they care so much about improved funding for medical research.
“As a protected, perpetual fund, the Australian Government’s MRFF will lead to many more medical discoveries and help us make our health system more effective and efficient by doubling the government’s investment in medical research.”
Scott hopes the website www.whatsthefuss.org.au will become a place where people can tell their personal stories, be they medical research success stories or about conditions that need more research.
“There are the people we’ve lost, such as our group’s founding chair, Alastair Lucas, who died of brain cancer recently. For him before he died, and for all who loved him, there was that crucial intangible that medical research delivers: hope. Hope for a treatment, for a cure. Hope is priceless.”
The Medical Research Future Fund is a protected, perpetual fund that is slated to build to $20 billion by 2020. At this point, it will deliver $1 billion in annual funding to medical research and innovation.
It’s been a chequered time for medical workforce planning in recent years.
Health Workforce Australia (HWA) was a Commonwealth statutory authority established in 2009 to deliver a national and co-ordinated approach to health workforce planning, and had started to make substantial progress toward improving medical workforce planning and coordination. It had delivered two national medical workforce reports and formed the National Medical Training Advisory Network (NMTAN) to enable a nationally coordinated medical training system.
Regrettably, before it could realise its full potential, the Government axed HWA in the 2014-15 Budget, and its functions were moved to the Health Department. This was a short-sighted decision, and it is taking time to rebuild the workforce planning capacity that was lost.
NMTAN is now the Commonwealth’s main medical workforce training advisory body, and is focusing on planning and coordination.
It includes representatives from the main stakeholder groups in medical education, training and employment. Dr Danika Thiemt, Chair of the AMA Council of Doctors in Training, sits with me as the AMA representatives on the network.
Our most recent meeting was late last month, and the discussions there make us hopeful that NMTAN is finally in a position where it can significantly lift its output, contribution and value to medical workforce planning.
In its final report, Australia’s Future Health Workforce, HWA confirmed that Australia has enough medical school places.
Instead, it recommended the focus turn to improving the capacity and distribution of the medical workforce − and encouraging future medical graduates to train in the specialties and locations where they will be needed to meet future community demands for health care.
The AMA supports this approach, but it will require robust modelling.
NMTAN is currently updating HWA modelling on the psychiatry, anaesthetic and general practice workforces. We understand that the psychiatry workforce report will be released soon. This will be an important milestone given what has gone before.
Nonetheless, it will be important to lift the number of specialties modelled significantly now that we have the basic approach in place, so that we will have timely data on imbalances across the full spectrum of specialties.
The AMA Medical Workforce Committee recently considered what NMTAN’s modelling priorities should be for 2016.
Based on its first-hand knowledge of the specialities at risk of workforce shortage and oversupply, the committee identified the following specialty areas as priorities: emergency medicine; intensive care medicine; general medicine; obstetrics and gynaecology; paediatrics; pathology and general surgery.
These have the potential to give future medical graduates some of the career information they will need to choose a specialty with some assurance that there will be positions for them when they finish their training.
Australia needs to get its medical workforce planning back on track.
Let’s hope that NMTAN and the Department of Health are up to the task.
The National Health and Medical Research Council (NHMRC) reports that it has opened a joint funding round with their American counterparts, the United States National Institutes of Health (NIH) as part of the United States Brain Research through Advancing Innovative Neurotechnologies (BRAIN) Initiative. Under this collaboration, the NHMRC will provide funding to support Australian researchers to participate in The BRAIN Initiative, which was announced by President Obama in 2013. “It is hoped that the research conducted through The BRAIN Initiative will lead to more effective treatments and methods of prevention for brain conditions such as dementia, autism, epilepsy, depression and Parkinson’s disease”, the NHMRC statement read. The NHMRC CEO Professor Anne Kelso said: “Both the NIH and the NHMRC believe that the ambitious goals of The BRAIN Initiative can best be attained by collaborating across both disciplinary and geographic boundaries. Over the past four decades Australian researchers have collaborated more with researchers in the US than in any other country.”
Missing microbes may point to asthma risk
NPR reports that a new study published in Science Translational Medicine shows that the composition of microbes living in babies’ guts may play a role in whether the children develop asthma later on. “The researchers sampled the microbes living in the digestive tracts of 319 babies, and followed up on the children to see if there was a relationship between their microbes and their risk for the breathing disorder … the researchers report that those who had low levels of four bacteria were more likely to develop asthma by the time they were 3 years old. To further test their theory, the researchers gave laboratory mice bred to have a condition resembling asthma in humans the four missing microbes. The intervention reduced the signs of levels of inflammation in their lungs, which is a risk factor for developing asthma.” The bacteria are from four genuses: Lachnospira, Veillonella, Faecalibacterium and Rothia.
“Predatory” journals publish 400k papers in 2014
Retraction Watch reports that a new analysis by BioMed Central shows that in 2014 so-called “predatory” open-access (OA) journals published around 420 000 papers, up from 53 000 in 2010, appearing in 8000 active journals. “Predatory” OA journals allegedly sidestep publishing standards in order to make money from article processing charges (APC). “Lately, most predatory journals are published by smaller publishers, which maintain between 10 and 99 titles”, Retraction Watch wrote. “The average APC was US$178, and most were published within 2–3 months after being submitted. Predatory journals have made the news — this year, The International Archives of Medicine was delisted from the Directory of Open Access Journals after it accepted a bogus study claiming chocolate had health benefits within 24 hours. In 2013, the same author behind that chocolate study, John Bohannon, tricked more than half of a sample of 300 OA journals to accept fake papers submitted under a fake name and institution. Last year, the Ottawa Citizen tricked a cardiology journal into publishing a paper with a garbled blend of fake cardiology, Latin grammar and missing graphs, for the price of US$1200.”
Cut and paste “tattoo” monitors health 24/7
An inexpensive wearable patch that continuously monitors vital signs for health and performance tracking has been developed by engineers in Texas, Futurity and Engadget report. The “tattoo” is manufactured via a repeatable “cut-and-paste” method that cuts production time from several days to only 20 minutes. “After producing the cut-and-pasted patches, the researchers tested them and discovered they picked up body signals that were stronger than those taken by existing medical devices, including an ECG/EKG, a tool used to assess the electrical and muscular function of the heart. The patch also conforms almost perfectly to the skin, minimising motion-induced false signals or errors. The wearable patches are so sensitive they may be worn to more easily maneuver a prosthetic hand or limb using muscle signals.”
Social network for doctors and their case photos
A new photo-sharing social network called Figure 1 is gaining popularity with doctors, nurses, paramedics and other medical workers, Wired reports. “Figure 1 is educational, engaging, and privacy-obsessed.” Anyone can join, but only health care professionals can comment on photos, which, says Wired, “keeps the discourse focused and professional”. The app is also heavily moderated. An image will be blocked if it doesn’t pose some kind of medical question. The app is very careful about patient privacy. “Every time anyone uploads an image, the first thing they do is fill out a consent form. Figure 1 has an algorithm that automatically obscures faces, and tools that let the user erase any pixels containing names, dates, or any other identifying details.” Figure 1 also strips away all the metadata before the picture gets uploaded. No data collection, over 500 000 users and so far, no ads. “Some of the pictures are straight up medical oddities. But just as often, users post because they are stumped and looking for a 2nd, 3rd, 4th, nth opinion.” The app is available from the iTunes App Store, Google Play and figure1.com.
Recognising health as its key engine of economic progress, China is undertaking an unprecedented and rapid health system transformation towards universal health coverage (UHC), since its ambitious health reform was launched in 2009. The Lancet has been tracking and monitoring the progress and challenges of China’s health reform through publishing its China Series and themed issues regularly since 2008, because we believe the lessons learned from China will have important implications for not only the country itself but also for the rest of the world.
Influential medical clinician and researcher, Laureate Professor Nicholas Talley, has been appointed as the new Editor in Chief of the Medical Journal of Australia.
AMPCo Board Chair Richard Allely said Professor Talley, who is currently Pro Vice Chancellor, Global Research, at the University of Newcastle and a part-time staff specialist gastroenterologist at the John Hunter Hospital, came to the position with a wealth of local and international experience in medical research, practice and publishing.
“Professor Nick Talley is a clinician, educator, writer, author, researcher, and editor, with a strong track record in medical practice, medical education, and medical publishing, in Australia and overseas,” Mr Allely said.
As well as having authored 800 original and review articles in peer-reviewed academic journals, Professor Talley is currently Co-Editor in Chief of the international journal Alimentary Pharmacology and Therapeutics (a position he will relinquish soon after he takes up the MJA post on 1 December), and served for six years as Co-Editor in Chief of the American Journal of Gastroenterology.
“He brings significant experience, knowledge and expertise to the MJA, and is perfectly suited to guiding Australia’s leading medical journal at a time of rapid change, innovation and technological revolution in media and publishing,” Mr Allely said.
In addition to his ongoing academic, clinical and publishing work, Professor Talley is President of the Royal Australasian College of Physicians and Chair-elect of the College of Presidents of Medical Colleges.
He also holds several international adjunct appointments, including Professor of Medicine and Professor of Epidemiology at the Mayo Clinic, and Foreign Guest Professor at Stockholm’s Karolinska Institute.
Professor Talley’s appointment was announced soon after it was revealed that AMA Federal Councillor and former Australian Medical Students’ Association President Jessica Dean had been recruited to the Board of mental health organisation beyondblue.
beyondblue Chairman Jeff Kennett said Ms Dean’s experience as a young doctor would be “invaluable” for his organisation as it sought to work with medical students and practitioners at risk of experiencing depression and anxiety.
Ms Dean has been a member of beyondblue’s Victorian Doctors’ Mental Health Advisory Group, and earlier this year addressed a meeting of senior Victorian doctors, health officials and administrators about the mental health of medical practitioners and the culture in which they work.