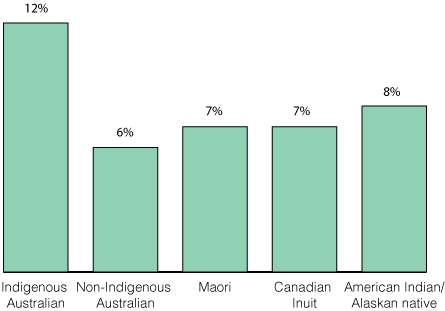
The disparities in health outcomes between Aboriginal and Torres Strait Islander (hereafter called Indigenous) and non-Indigenous Australians are well established, with the life expectancy gap being among the worst in the world.1 There is growing evidence that the chronic diseases that are prevalent in Indigenous Australian adults (diabetes, hypertension, cardiovascular and renal disease) have their genesis in utero and in early life.2,3 One of the greatest medical threats to the wellbeing of Indigenous children is being born preterm or at a low birthweight (LBW). Australian Indigenous babies are almost twice as likely to be born LBW than Australian non-Indigenous babies or Indigenous babies from similar countries (Box). Other contributors to poor outcomes include the enduring effects of colonisation, social exclusion, sustained institutionalised racism, and stark inequities across many of the social determinants of health, including income, employment, education, and access to goods, services and health care.6,7
Australia’s National Maternity Services Plan (NMSP) states that Australia is “one of the safest countries in the world in which to give birth or to be born. However, this is not the case for Aboriginal and Torres Strait Islander people.”8 The NMSP was based on an extensive review of maternity services.9 It set out a 5-year vision for the years 2010–2015, and a framework for implementation with the federal, state and territory governments endorsing the plan and committing to long term improvements, investments and service developments under four key areas: access, service delivery, workforce and infrastructure. Actions for the initial, middle and later years were identified, as were indicators to measure the signs of success. The NMSP identified three priority areas for Indigenous women: (i) increasing the Indigenous workforce; (ii) increasing culturally competent maternity care; and (iii) developing dedicated programs for Birthing on Country.8
We reviewed government documents that are freely available and related to the NMSP, including annual reports.10–12 We included relevant literature published since the release of the Review of Maternity Services in 2009,9 and other literature related to maternity services for Indigenous women. We examined the four key areas in relation to the priority areas for Indigenous women. We note that the NMSP did result in additional benefits to all Australian women that are not detailed in our review, for example the development of the National Evidence-Based Antenatal Care Guidelines.
Priority 1: The Indigenous maternity workforce
Action 3.2 of the NMSP was to develop and support an Indigenous maternity workforce across all disciplines and qualifications, and to provide more scholarships (such as the Puggy Hunter Memorial Scheme) to facilitate this action. Small one-off initiatives are seeing slow progress in this area with some jurisdictions doing better than others. In 2015, there were 230 Indigenous midwives nationally, comprising only 1% of the midwife population, while Indigenous Australians constitute 3% of the population and 6% of all Australian births.13 Additionally there is a marked drop-out of midwifery graduates from clinical roles soon after graduation, and this highlights a need for ongoing support.14
Across Australia, we are seeing an increasing number of maternity models that recognise the contribution of Indigenous workers who have a variety of titles and job descriptions. Some recognise the importance and cultural expertise of elders and grandmothers like the Strong Women Workers,15 while others aim to provide women support through bicultural partnerships between midwives and maternal infant health workers,14–19 with some supporting Indigenous student midwives (Appendix). This is a positive start that needs dedicated funding for scaling up and monitoring. In Canada, the Inuit have managed this in very remote settings,20 but we see little of this in Australia. Increasing the Indigenous workforce is likely to increase the cultural competence of the whole workforce and the workplace.14
Priority 2: Culturally competent maternity care
Action 2.2 of the NMSP was to develop and expand culturally competent maternity care for Indigenous Australians. Cultural competency is best comprehended as a philosophy and paradigm for transformational heath practice. Importantly, the ideologies with cultural competence, safety, security and respect are to embed knowledge, skills and values to create change to enable culturally responsive and informed care. Evidence from America has shown that the use of this approach in government-funded agencies has improved the knowledge and attitudes of health professionals working with clients from marginalised groups, whose disparities are costing health services greatly.21 The NMSP tackled this by commissioning a literature review to document the characteristics of culturally competent maternity care and draft indicators for measurement.22 Further work was to develop mechanisms for evaluating cultural competence in maternity care and undertake a national stocktake of access to culturally competent maternity care; both have yet to be completed. However, the establishment of the National Centre for Cultural Competence, a joint venture of the Australian Government and the University of Sydney, is likely to have an impact nationally with online and workshop cultural competency training and resources available for a broad audience. Additionally, the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives provide face-to-face health-specific training in cultural safety.
Cultural competency education and training is a strategy aimed at addressing health disparities, although further development and work are required to appreciate the most effective methods, the flow-on effect of training to patients, and the best tools for measuring cultural competence in individuals, organisations and in the maternity setting.21–23 Critically, “racism constitutes a ‘double burden’ for Indigenous Australians, encumbering their health as well as access to effective and timely health care services.”24 Achieving culturally competent maternity services is key to improving maternity care and good health for mothers and babies.25
Another emerging area in developing a cultural competent workforce is that of trauma-informed care and practice, whereby care providers understand the ongoing impact of intergenerational trauma resulting from historical injustices, colonisation, removal from and dispossession of land, and continuing racism.26 This is particularly important given that Indigenous children are overrepresented in out-of-home care compared with non-Indigenous children (nine times higher; 35%27), with some women encountering the child protection system during pregnancy, leading to the removal of their babies at birth. This is an incredibly distressing situation for all involved, but most particularly the mother. Redirecting funding from removal to supporting vulnerable families would see greater short and long term benefits.
Although maternity services in Australia are designed to offer women the best care, they largely reflect modern western medical values and perceptions of health, risk and safety.28 This is unlike the Indigenous world view, reflected in their definition of health, which incorporates not just physical wellbeing, but also the social, emotional and cultural wellbeing of individuals and the whole community.7
Maternity systems have failed to incorporate the evidence provided by Indigenous women on the impact of social risks that include cultural risk (eg, the belief that not being born on their land threatens claims to land rights) and emotional risks (having to spend weeks removed from family and other children while awaiting birth).29,30 Recent empirical work in Australia reconfirms that these risks are still valid, highlighting that they not only cause distress to women and families, but also increase clinical and medical risks (eg, women not attending antenatal care, or presenting late in labour, to avoid being flown out of their community for birth); this is a factor not well understood by health service leaders.28 The risks are greater for Indigenous women from remote and very remote communities, some of whom feel that giving birth in hospitals, many miles from their home, may be the cause of ill health as it breaks the link between strong culture, strong health and the land, a link that is strengthened during birth.31 While away from community and other children awaiting the birth, pregnant women are susceptible to anxiety, stress and depression, and often have particular concerns that their other children may be vulnerable to child protection services in their absence.30
We acknowledge the importance of clinical and medical risk, but suggest that the definition of risk needs be broader, to incorporate the social (cultural, emotional and spiritual) risks as valid and important dimensions of risk assessment requiring risk management processes. For example, when women need to leave their community for specialist care, strategies to ensure her other children are safe, or can travel with her, must be implemented as part of the risk management process. The disconnection between social, cultural and spiritual risk and western clinical and medical biophysical risk is a critical and understudied phenomenon that needs further work.
Priority 3: Dedicated programs for “Birthing on Country”
Action 1.4 of the NMSP was to increase access to high quality maternity care for women and their family members in remote Australia. Twenty-four per cent of Indigenous women who give birth each year live in remote and very remote Australia (versus 2% of non-Indigenous women), highlighting the importance of services in these areas. Although there has been some improvement in pregnancy care in some communities,32 empirical studies continue to report the challenges of providing maternity services in these areas, a lack of regular access to midwifery care and suboptimal quality of care caused by the lack of a systematic approach, appropriate clinical governance and cultural competence among health care providers.18,33,34 One approach to solving this in some of the larger remote and very remote communities is to establish Birthing on Country sites.
Action 2.2.3 of the Plan addressed Birthing on Country, which was defined as maternity services designed and delivered for Indigenous women that encompassed some or all of the following elements:
-
were community based or governed;
-
incorporated traditional practice;
-
recognised the connection with land and country;
-
incorporated a holistic definition of health;
-
valued both Indigenous and non-Indigenous ways of knowing, learning and risk assessment; and;
-
were culturally competent and developed by, or with, Indigenous people.35
The Maternity Services Inter-Jurisdictional Committee brokered a literature review of Birthing on Country programs in Australia, New Zealand, Canada and America to determine if any had made a significant improvement to outcomes. The review found a number of programs met the criteria, but there was a dearth of high quality research, with most studies having short term evaluations, small numbers and potential selection bias. Despite this, some programs show significant improvements in antenatal attendance, screening and treatment; immunisation rates; mean birth weight; reduced preterm birth and cost; and women report increased satisfaction (see full report35 for details, and the Appendix to this article for examples).
The Inuit model in Northern Quebec provided the most robust evidence of an “exemplar model”, where three Birthing on Country services operate in places that are many hours by plane from facilities where caesarean delivery can be performed. These facilities meet community expectations, address clinical/medical, social/cultural, spiritual and emotional risks and have improved maternal and infant health outcomes while supporting local midwifery training.20 Increasing numbers of these services are operating in Canada, with some having been sustainable since the mid-1980s and early 1990s.20 The benefits of community-based birthing services, over and above the improvements in maternal infant health outcomes, include community healing, comprehensive tailored care, support of the community, local training and employment and reduced family separation at critical times.20 The evidence suggested that a Birthing on Country model of maternity care would most likely produce significantly improved outcomes for Indigenous women in very remote through to urban areas.35
The review was followed by a national Birthing on Country workshop, facilitated by the Maternity Services Inter-Jurisdictional Committee and Congress Alukura in Alice Springs in 2012. Participants voiced concern that “Birthing on Country”, as a term, lacked clarity which may have contributed to a lack of engagement from key service providers and government departments. Nevertheless, participants proposed that Birthing on Country be retained and understood as “a metaphor for the best start in life for Aboriginal and Torres Strait Islander babies and their families, an appropriate transition to motherhood and parenting for women, and an integrated, holistic and culturally appropriate model of care.”36 The middle and later years of the NMSP were to see Birthing on Country programs developed and evaluated, with the workshop recommending that “exemplar sites” be established in urban, rural, remote and very remote areas to deliver “… not only bio-physical outcomes … it’s much, much broader than just the labour and delivery … [Birthing on Country] deals with socio-cultural and spiritual risk that is not dealt with in the current systems”36
Birthing on Country in remote and very remote Australia
Despite policy frameworks that support primary maternity services delivering culturally competent care closer to home,7,8,37 demand from Indigenous women and communities,38,39 and multiple recommendations over 25 years,8,38–41 there has been no progress towards establishing and evaluating Birthing on Country services in remote or very remote Australia. In these areas, such services would need to be Primary Maternity Units or Services, which are defined in the National Maternity Services Capability Framework42 (Action 4.2.2 of the Plan saw the development of this Framework) as Level 2 services. Internationally, there is strong empirical evidence that Primary Maternity Units/Services provide safe perinatal care for women classified as being at low risk of complications,43,44 including in rural and remote areas.20,45 Despite this, few such services operate in Australia (3 urban/regional; 17 rural; 0 remote),46 reflecting a centralisation of services, a lack of medical support in some cases, safety and sustainability concerns in others.44,47 In fact, Australia has seen a 41% decline in maternity services over the 20 years from 1992 to 2011, especially in rural areas, correlating with a 47% increase in unplanned out-of-hospital births (22 814 births).48 There is an unequivocal relationship between distance to maternity services and poorer clinical49 and psychosocial outcomes.50,51 This lends support to the argument to prioritise Birthing on Country models in remote and very remote areas, where some of the most disadvantaged women in Australia live the furthest from maternity services.
Determining the appropriate level of maternity services that are safe and will be sustainable in a given location is challenging. Action 4.2.1 in the NMSP was to develop rigorous methods to help with planning maternity care in rural and remote communities. This work was completed with the development of the Australian Rural Birth Index, which can be used to determine the appropriate level of maternity service for a community, based on the average number of births in a community, the vulnerability of the community, and distance to a facility that can perform caesarean delivery.52 The work accompanying this project found disparities in access to services across Australia and minimal adjustment for the needs of vulnerable, rural and remote populations. Additionally, the project identified that the perceived risks to health services of operating services in remote areas is given priority over the clinical and social risks experienced by families (when they do not have local maternity services).28
Where to from here?
The Review of Maternity Services outlined serious challenges that needed attention in Australia and recognised a clear role for leadership by the Australian Government in concert with state and territory governments.9 The NMSP was developed to address these issues and to measure progress.8 There is little doubt that it resulted in the strengthening of maternity services in some areas. Additionally, three National Health and Medical Research Council Partnership projects are advancing Birthing on Country in urban areas. In Perth, there is a project exploring the Cultural Security of Aboriginal Birthing Women;53 in Melbourne, the Aboriginal Community Controlled Health Organisations (ACCHOs) and three large hospitals are offering all Indigenous women one-on-one midwifery care with a known midwife antenatally, in labour and up to 6 weeks postnatally;54 and, in Brisbane, one of us (S K) is working with two ACCHOs and two large maternity hospitals to develop and evaluate an Urban Birthing on Country service model. Several jurisdictions are developing models incorporating some of the principles of Birthing on Country; most are successfully engaging pregnant women earlier and more often than standard care, and early evaluations are starting to show improved outcomes (Appendix).
We must not lose this momentum. It is time for a new maternity services plan with high level monitoring to continue to tackle emerging priorities and complete unfinished business, particularly for Indigenous women in rural and remote communities. Three professional organisations (the Australian College of Midwives, the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives and the Remote Health Organisation, CRANAplus) have released a position statement calling for action,55 and recommending the Australian government show leadership and develop a strategic approach to implementing and evaluating Birthing on Country programs. We believe that leadership in this area must continue to come from the Australian government, with greater urgency than has been evident to date. Dedicated funding must be allocated towards supporting the Indigenous maternity workforce, developing and measuring culturally competent care and establishing Birthing on Country sites in urban, rural and particularly in remote and very remote communities. This recommendation is based on international evidence that already exists, and government funding should extend to generating further evidence so the lessons learned can be applied to sites elsewhere.