In Australia, 300 000 women give birth each year, with almost all using maternity care services, either public or private.1 Maternity services are the third most common specialised service offered by hospitals,2,3 accounting for more than one million patient-days annually.4 The most common principal diagnosis for overnight hospital stays is single spontaneous birth, which accounts for 4.2% of acute separations in public hospitals and 2.4% in private hospitals.4
The provision of high quality maternal and newborn care is an important global aim, as articulated by the United Nations.5 In Australia, the 2011 National Maternity Services Plan stated that “All Australian women will have access to high-quality, evidence-based, culturally competent maternity care in a range of settings close to where they live” and recognised that continuity of care is very important for women.6 This plan followed the Maternity Services Review, which made recommendations regarding access to a range of models of maternity care, with a focus on women in rural and remote areas and Aboriginal and Torres Strait Islander women, and the need to build and support the maternity workforce to ensure the provision of safe, quality care for all women.7
Much has happened in Australia and globally over the past decade in the provision of maternal and child health services, and specifically regarding models of maternity care. Here, my aim was to review the current evidence for models of maternity care that provide midwifery continuity of care, in terms of their impact on clinical outcomes, the views of midwives and childbearing women, and health service costs. I used PubMed to identify original studies and review articles for the past 15 years (2001 onwards), as well as national policy reports and guidelines, to formulate an evidence-based overview of midwifery models of care and their application in the maternity care system. The key search terms included midwife, midwifery continuity of care, continuity of carer, midwife-led and midwifery services. I also searched the reference lists of identified articles for further studies.
What are models of maternity care?
To review the evidence for midwifery models of care, an understanding of how such models are defined is first needed. “Models of maternity care” is a term frequently used but poorly understood. An extensive literature review undertaken by the Australian Institute of Health and Welfare found that models of care in general are poorly defined.8,9 One definition of a model of care is “an overarching design for the provision of a particular type of health care service that is shaped by a theoretic basis, EBP [evidence-based practice] and defined standards”.10
Models of maternity care can be provided in both the private and public sectors by obstetricians, general practitioners and midwives. In Australia, the Maternity Services Review defined maternity services as essentially falling within one of four broad models of care: private maternity care, combined maternity care, public hospital care and shared maternity care.6 However, there are many more nuances in the way maternity models of care are configured, depending on the sector (public or private), the risk status of the pregnant woman (low risk, high risk, or mixed), the carer (midwife, doctor, Aboriginal health worker), the way care is organised (caseload, collaborative links), the location (hospital, community, home) and the way women move through the model from entry to exit.8 To deal with these complexities, a national project has been developing a classification system for models of maternity care.11,12 This project has identified the major categories of models of care, including midwifery models of care that provide continuity of care (Box). Midwife-led continuity of care models include midwifery group practice caseload care, team midwifery care and private midwifery care. Midwifery group practice caseload care and team midwifery care are the focus of this review.
Midwifery continuity of care models: the evidence for benefit
In the past two decades, considerable research has been undertaken into models of maternity care that provide midwifery continuity of care. A Cochrane review of midwife-led continuity of care models included 15 randomised controlled trials involving 17 674 mothers and their babies.13 Seven of these trials were undertaken in Australia: in New South Wales,14–17 Victoria18,19 and Queensland.15,20 All 15 trials included women receiving care from licensed professional midwives, in collaboration with doctors where necessary. In most trials, the women were predominantly at low risk of obstetric complications, although in one of the more recent trials, conducted in Sydney and Brisbane, women were of a mixed obstetric and medical risk status and were not transferred out of the model if they developed further risk factors.15 Trials that included homebirth were excluded. A possible limitation of this Cochrane review is that it examined both team midwifery and caseload models, as it is not yet clear which model is most effective.
The findings showed benefits and no adverse effects compared with other models of care.13 Women who received midwife-led continuity of care were more likely to have a midwife they knew with them during labour and birth, more likely to have a spontaneous vaginal birth and less likely to have epidural analgesia, episiotomies or instrumental births. Women were less likely to experience a pre-term birth, and their babies were at a lower risk of dying (including all deaths before and after 24 weeks’ gestation and neonatal deaths). Women rated midwife-led continuity of care models highly in terms of satisfaction and there was a trend towards a cost-saving effect for the midwife-led models, although there was inconsistency in reporting of both these outcomes.13 The review concluded that “most women should be offered midwife-led continuity models of care”. While some trials included women of mixed risk who were cared for in collaboration with doctors, more research is needed to determine the most effective models of care for women with existing serious pregnancy or health complications. In addition, the included trials were all from high income countries, making generalisations to the context of low to middle income countries difficult.
The Cochrane review of midwife-led continuity of care models was one of the reviews analysed to develop a framework for quality maternal and newborn care for The Lancet’s Midwifery Series.21,22 The framework emphasised the centrality of midwifery continuity of carer in providing the care that is needed by women and newborn infants, regardless of setting, and highlighted the importance of working collaboratively in interdisciplinary teams to provide care for women and infants who have, or develop, complications.23
Midwifery continuity of carer has also been examined in non-randomised studies, although these carry an inherently increased risk of bias. These include a study in a large referral centre in Sydney, where a third of pregnant women received care through a midwifery continuity of care (caseload care) model.24 Midwives were organised in groups of four and were responsible for the care of a specified caseload of women throughout pregnancy, birth and the post partum period.25 The midwives followed the Australian College of Midwives’ National midwifery guidelines for consultation and referral.26 In this study, a “standard primipara”, defined as a first time, “low-risk” mother, was used as the unit of comparison, to reduce differences between the caseload care, standard hospital care and private obstetric care groups. Women who received caseload care were more likely to have a spontaneous onset of labour and an unassisted vaginal birth and less likely to have an elective caesarean delivery than those in the other two groups, with lower average costs of care.24
Midwifery continuity of carer can also be provided in “free-standing midwifery units”. In these units, primary level care is provided by a named midwife, with no routine involvement of medical staff. The units are geographically separate from the referral centres that provide obstetric, paediatric or specialised medical consultations when necessary. Free-standing midwifery units do not provide epidural analgesia or caesarean deliveries on site. A prospective cohort study of two such units in NSW showed that women who planned to give birth at a free-standing midwifery unit were more likely to have a spontaneous vaginal birth, less likely to have a caesarean delivery and had no differences in 5 minute Apgar scores compared with women who planned to give birth in tertiary level maternity units.27 Babies from the freestanding midwifery unit group were significantly less likely to be admitted to neonatal intensive care or the special care nursery. However, only two such units exist in Australia, suggesting that widespread implementation would be a challenge. Although this study analysed where mothers intended to give birth rather than where they actually did give birth, this accurately reflects the need for transfer in some women, and analysing according to intention is important in studies on place of birth. There was some crossover between the groups in actual birth locations, but these involved only 1% of the study population.
Across Australia, similar clinical and cost outcomes have been reported from non-randomised studies of midwifery continuity of carer in South Australia,28 Queensland29 and NSW.30 A review of 22 international non-randomised studies has also shown that low risk women in midwife-led, birth centre or homebirth services in the care of midwives experienced fewer obstetric interventions and were more likely to have a normal birth without complications than low risk women receiving standard hospital or obstetric care.31 Although these were non-randomised studies, with diverse study designs and models of care, they nevertheless provide additional evidence supporting midwifery continuity of care.
Midwifery models of care for specific groups
Midwifery models of care have been implemented for a range of specific groups, especially young women and women from minority or marginalised groups. For example, a retrospective cohort study in Queensland showed that women younger than 21 years of age who were allocated to midwifery continuity of carer (caseload care) were less likely to have a pre-term birth or to have their baby admitted to a neonatal intensive care unit than those receiving standard care.32
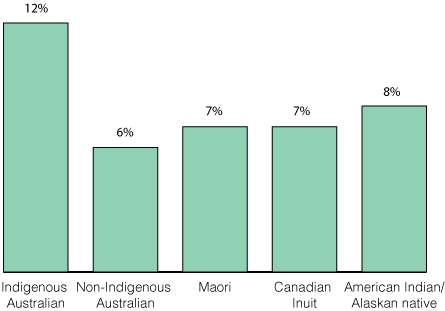
In Australia, Aboriginal and Torres Strait Islander women and babies experience higher maternal and perinatal morbidity and mortality rates than their non-Indigenous counterparts.1 Several models that provide midwifery continuity of carer have been specifically designed and evaluated for Aboriginal and Torres Strait Islander women.
In the Northern Territory, two such midwifery models have been evaluated. A midwifery group practice in Alice Springs catered for 763 local women, 40% of whom were Aboriginal, over 4 years. This model of care has eight midwives who work in pairs or teams of three, depending on skill level and work hours. Each pregnant woman is assigned a primary midwife, with back-up from her primary midwife’s colleagues, who she meets during her pregnancy. A retrospective review found that the rates of perinatal mortality, pre-term birth and low birthweight babies for these women were lower than those reported for the NT population.33 Retrospective analysis such as this has inherent limitations due to the nature of the data and the ability to make comparisons; however, a randomised controlled trial would not have been feasible or possible in this setting.
The other study in the NT involved a new model of maternity care for remote-dwelling Aboriginal women, who were transferred to a regional centre in Darwin to await birth. Women were provided with midwifery continuity of care from their arrival in Darwin until their transfer back home, with effective communication networks between the regional centre and remote community health centres. The study showed that, for the first time, Aboriginal women could access continuity of care once they reached Darwin, and the women reported more positive experiences with maternity services than previously.34 The model was shown to be cost-effective for remote-dwelling Aboriginal women of all risk levels.35
In a more urban setting, a midwifery continuity of carer model was established in an area of high socio-economic disadvantage in Sydney, to meet the needs of Aboriginal women and families, as well as non-Aboriginal women and families from nearby suburbs, many of whom were from migrant and refugee communities.36 The service was based in a suburban house 6 km from the referral hospital. Women received antenatal care and postnatal or child health services from the house and gave birth in the labour ward of the referral hospital. The service was staffed by midwives, Aboriginal health education officers, a community health worker and a child and family health nurse. The midwives and Aboriginal health education officers accompanied the women to the hospital if they needed to attend for antenatal visits, and the midwives were on call to care for the women when they went into labour. An evaluation of qualitative and quantitative data showed that women and the local community valued the service and that women were likely to attend for antenatal care early in pregnancy and to engage with health promotion initiatives, such as smoking cessation.36 Continuity of caregiver (midwife and Aboriginal health education officer) was highlighted, with women in the focus groups speaking of this aspect as being “the best part” of the service.
Midwifery continuity of care: effect on organisations and midwives
In both the public and private sectors, midwifery continuity of care is usually provided in a caseload model. These midwives work on call rather than on a shift-based roster and usually have arranged times for antenatal and postnatal care (provided either in hospital or community settings or women’s homes). The midwives usually work in partnerships or small groups to enable care by a back-up midwife who is known to the woman, should her primary midwife be unavailable.37,38 They also work within hospital guidelines and collaborate with non-caseload midwives, managers, obstetricians and other medical specialists as required. In Australia, a full-time caseload midwife in a public hospital model cares for 30–40 women per year as the primary midwife (depending on the complexity of the women’s pregnancies) and provides back-up for colleagues who usually have a similar caseload.39 Industrial guidelines, which vary across the country, ensure that midwives have adequate time off and are fairly remunerated for their on-call work.
Some midwifery continuity of carer models are based in birth centres, while others use the hospital’s standard labour ward. There are a few models that also provide access to publicly funded homebirth for carefully screened women at low risk of complications.40,41
Midwifery continuity of carer, or caseload midwifery, has been associated with positive outcomes for midwives. Research from Victoria showed that caseload midwives had lower burnout scores and higher professional satisfaction than midwives who worked in standard shift-based ways.42 This was a small study from one setting, but similar findings have also been reported from Adelaide,43 the United Kingdom44 and New Zealand.45 In a recent qualitative study in Australia, newly graduated midwives who were supported, mentored and orientated reported considerable benefits from working in midwifery continuity of care models and were highly satisfied with their work.46,47
Translating this evidence into practice
Currently in Australia, although midwifery continuity of care and carer is espoused in many state48 and national6 policy documents, with “toolkits”49,50 and guidance39 also available, widespread implementation remains limited. A recent national survey aimed to determine the prevalence of and factors associated with implementation and sustainability of midwifery models of care, especially caseload midwifery services.51 Participants were the maternity managers of the 235 public hospitals that provide birthing services. The survey had a 63% response rate (149/235), representing all states and territories; metropolitan, regional and remote areas; and hospitals with very small to very large birth numbers. Only 31% of responders reported that their hospital offered caseload midwifery, with an estimated 8% of women receiving caseload care at that time. Of those hospitals without a caseload model, 62% reported that they were planning to establish one. The survey showed that midwifery continuity of care models were expanding across the country and that there was strong perceived consumer interest in such models. Most hospitals with a caseload model reported having more women who wanted to access this model than there were places available, and community demand was high in areas where implementation was being considered.51 The findings of this study are clearly limited by its response rate of 63%, and further research examining the models of midwifery care available in Australia is needed to quantify the translation of evidence into practice.
Despite this survey’s limitations, it is clear that midwifery continuity of carer is not being widely implemented in Australia. Factors contributing to this include a lack of midwifery and medical leadership, workforce shortages and fears about the autonomy of midwives. A lack of medical staff support continues to be cited as an obstacle to change in many services.51 Nevertheless, some services have been developed through effective and respectful collaboration between midwives and doctors, and there is evidence that such interprofessional collaboration is attainable in midwifery continuity of care models.52
Recruiting and retaining midwives who are interested in and available for work in this model remain problems for many services. However, all new graduates from Australian midwifery programs have had opportunities to work in this way during their education,53 and many want to work this way in the future.54 Midwifery continuity of care is a “different” way of working, and it takes time for midwives and their managers to adapt to working on call, with fewer boundaries between work and personal time.38 This is not always embraced by service managers, medical staff or hospitals, as it requires trusting the midwives and enabling them to develop professional relationships with women and to assume responsibility, accountability, autonomy and legitimacy in their practice.38
Many hospital managers raise concerns about the effects of staff burnout on the sustainability of midwifery continuity of care models.55 Despite this, research in the UK has shown that high levels of occupational autonomy and assistance with ensuring a work–life balance provide a protective effect on the levels of burnout for midwives.56
Models of midwifery care for the future
Globally, the understanding that midwifery models of care are best practice for all pregnant women is gathering momentum. The evidence is now clear; there is Level I evidence from well conducted randomised controlled trials showing benefit for women and the health system, and numerous non-randomised studies show similar benefits for women, midwives and organisations. Recent international policy documents highlight the need for midwifery continuity of carer. For example, the 5-year forward view for maternity care in England, known as “Better Births”, recommends:57
Continuity of carer, to ensure safe care based on a relationship of mutual trust and respect in line with the woman’s decisions. Every woman should have a midwife, who is part of a small team of 4 to 6 midwives, based in the community who knows the woman and family, and can provide continuity throughout the pregnancy, birth and postnatally.
The Australian maternity care system is similar to that in the UK, and this recommendation was based on evidence partly drawn from Australian studies.13
To bridge the gap in translating the evidence into clinical practice in Australia, widespread reorganisation of the way maternity services are provided is required. Midwifery continuity of carer programs can no longer be implemented as pilot programs or in piecemeal ways for small numbers of women; the evidence and the demand are now so strong that widespread reform is needed. A critical part of such reform is effective collaboration with obstetricians, general practitioners, paediatricians and other medical professionals involved in the care of pregnant women. Enabling and facilitating midwives to take a lead role in the care of women is an essential step in the process of reforming the maternity care system. A better understanding of the barriers and challenges associated with implementing midwifery continuity of care is also needed, and further research should examine this research–practice gap.
Despite the need for more research into ways to effectively implement this model of care in practice, is it ethical to withhold access to midwifery continuity of care from the majority of women in Australia, given the strength of evidence, the supporting policy documents and the demand from women? Future models of maternity care in Australia need to ensure that women have access to midwifery continuity of care. Midwives need to be valued and respected in their roles as key providers of primary maternity services in all settings for childbearing women in Australia. Flexible ways of working need to be enabled so that midwives can provide continuity of care, and innovative funding models in the public and private sectors need to be developed so that women can access the maternity care provider they need and want.
Box –
Identified major categories of models of maternity care in Australia11
|
Model of care category
|
Description
|
|
|
Midwifery group practice (public) caseload care
|
Antenatal, intrapartum and postnatal care is provided by a known primary midwife with a secondary back-up midwife or midwives providing cover, and with assistance from doctors where needed.* Antenatal and postnatal care is provided in the hospital, community or home, with intrapartum care in a hospital, birth centre or home.
|
|
Team midwifery care
|
Antenatal, intrapartum and postnatal care is provided by a small team of rostered midwives, in collaboration with doctors where needed.* Intrapartum care is usually provided in a hospital or birth centre. Postnatal care may continue in the home or community, provided by the team midwives.
|
|
Private midwifery care
|
Antenatal, intrapartum and postnatal care is provided by a private midwife or group of midwives, in collaboration with doctors where needed.* Intrapartum and postnatal care is provided in a range of locations, including at home.
|
|
Shared care
|
Antenatal care is provided by a community provider (doctor and/or midwife) in collaboration with hospital staff under an established agreement. Intrapartum and early postnatal care is usually provided in the hospital by hospital midwives and doctors, often in conjunction with the community provider (particularly in rural settings).
|
|
Combined care
|
Antenatal care is provided by a private maternity service provider (doctor and/or midwife) in the community. Intrapartum and early postnatal care is provided in the public hospital by hospital midwives and doctors. Postnatal care may continue in the home or community, provided by hospital midwives.
|
|
Private obstetrician (specialist) care
|
Antenatal care is provided by a private specialist obstetrician. Intrapartum care is provided in a private or public hospital by the private specialist obstetrician and hospital midwives. Postnatal care is provided in hospital and may continue in the home or a hotel.
|
|
Private obstetrician and privately practising midwife joint care
|
Antenatal, intrapartum and postnatal care is provided by a privately practising obstetrician and midwife from the same private practice. Intrapartum care is provided in either a private or public hospital by the privately practising obstetrician, midwife and/or hospital midwives. Postnatal care is provided in hospital and may continue in the home, hotel or hostel, provided by the private midwife.
|
|
General practitioner obstetrician care
|
Antenatal care is provided by a GP obstetrician. Intrapartum care is provided in a private or public hospital by the GP obstetrician and hospital midwives. Postnatal care is provided in the hospital by the GP obstetrician and hospital midwives and may continue in the home or community.
|
|
Public hospital maternity care
|
Antenatal care is provided in hospital outpatient clinics (onsite or outreach) by midwives and/or doctors. Intrapartum and postnatal care is provided in the hospital by midwives and doctors. Postnatal care may continue in the home or community, provided by hospital midwives.
|
|
Public hospital high risk maternity care
|
Antenatal care is provided to women with medical high risk or complex pregnancies by maternity care providers with an interest in high risk maternity care (specialist obstetricians or maternal–fetal medicine subspecialists with midwives) in a public hospital. Intrapartum and postnatal care is provided by hospital doctors and midwives. Postnatal care may continue in the home or community, provided by hospital midwives.
|
|
Remote area maternity care
|
Antenatal and postnatal care is provided in remote communities by a remote area midwife (or a remote area nurse) or group of midwives, sometimes in collaboration with a remote area nurse and/or doctor, with telehealth or fly-in–fly-out clinicians. Intrapartum and postnatal care is provided in a regional or metropolitan hospital (involving temporary relocation before labour) by hospital midwives and doctors.
|
|
|
* Collaboration with doctors “where needed” means “in the event of identified risk factors”.
|