
Iron deficiency remains one of the most common nutritional deficiencies worldwide and Australian women are at risk. Anaemia is a late sign of iron deficiency and many women experience symptoms before a decline in haemoglobin is detected. Common early symptoms of iron deficiency include fatigue, poor concentration and irritability.
Iron is an essential mineral for haemoglobin production, oxygen transport, DNA synthesis and muscle metabolism. The body cannot produce iron, making dietary intake critical.
To help educate on iron, MLA Healthy Meals has developed evidence based nutrition resources for patients available online at https://www.mlahealthymeals.com.au/.
The Current Situation in Australia
- Prevalence: The World Health Organization (WHO) reports globally, 30% of women aged 15–49 years have anaemia and in Australia, 11% of women non-pregnant and 14% of pregnant women are anaemic. It is estimated that nearly half of pregnant Aboriginal and Torres Strait Islander women experience iron deficiency anaemia.
- Iron Stores: The Australian Bureau of Statistics (ABS) reports Australian teenage girls have median ferritin levels around 25 µg/L, indicating insufficient iron stores. Among women aged 18–39, 35–37% have ferritin <30 µg/L, often linked to heavy menstrual bleeding (here and here).
- Dietary Intake: The latest National Nutrition survey revealed women consume about 50% less iron than the recommended daily intake (RDI).
- Teenage girls: RDI 15 mg/day vs actual ~9 mg/day
- Women 19–50 years: RDI 18 mg/day vs actual ~8.5–9 mg/day
- Pregnancy: RDI 27 mg/day (intake data unavailable)
- The National Health and Medical Research Council (NHMRC) notes that Vegetarians require 80% higher iron intake due to lower bioavailability.
Why Are Women at Risk of Iron Deficiency?
- Blood Loss: Heavy menstrual bleeding is the leading cause of iron deficiency in Australia. Women typically lose around 40-50ml of blood, equating to ~25 mg of iron per cycle. Between 25-53% of women experience heavy menstrual bleeding and are more likely to report symptoms of iron deficiency and have a history of an anaemia diagnosis (here and here).
- Physiological Demands: Children, adolescents, pregnant women and athletes have increased iron needs to meet growth demands and risk factors are a low iron intake.
- Dietary Patterns: Lower iron intakes mainly from non-haem sources (fortified cereals and grains) that are not as bioavailable as haem sources.
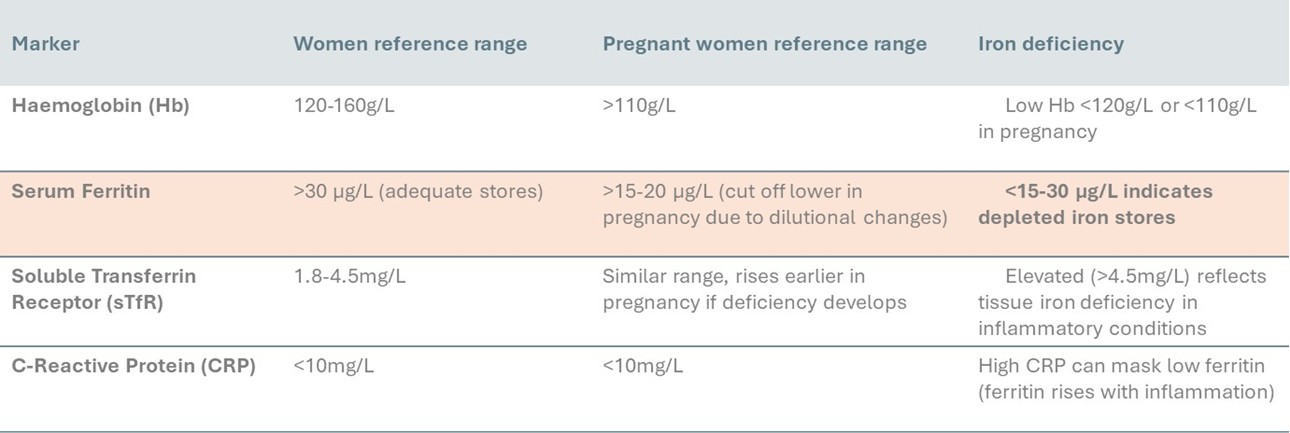
Iron Deficiency Diagnosis
- Ferritin <30 µg/L indicates insufficient stores.
- Haemoglobin <120 g/L (or <110 g/L in pregnancy) suggests anaemia.
- Consider serum transferrin receptor and CRP for complex cases.
How GPs Can Help
1. Screen and Diagnose
- Ask women about fatigue, heavy menstrual bleeding and dietary iron intake.
- Use screening questions for heavy menstrual bleeding.
- Encourage routine ferritin checks for women with symptoms or in high-risk groups.
2. Educate Patients
- Explain haem vs non-haem iron and absorption strategies:
- Pair iron-rich foods with vitamin C.
- Limit inhibitors like tea, coffee, and calcium around iron-rich meals.
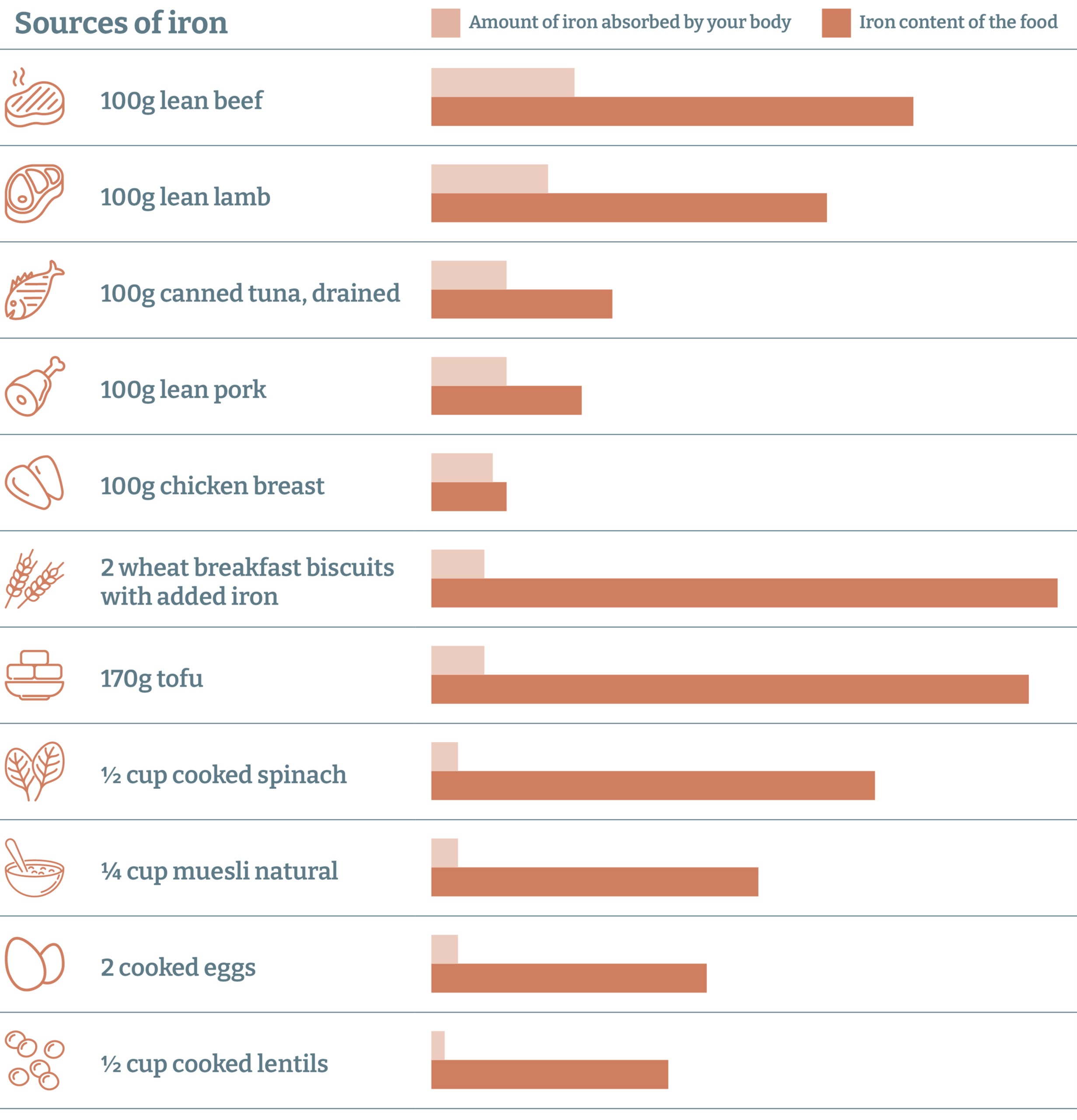
Dietary iron is available in two forms: haem iron, which is found in animal sources (red meat, and to a lesser extent poultry and fish), and non-haem iron, which is the only form of iron available in plant sources (nuts, cereals, beans and vegetables – particularly leafy greens). Absorption varies with iron status and meal composition. On average 25% of haem iron is absorbed, compared with 10% of non-haem iron. The percentage of non-haem iron absorbed increases as body iron stores decrease. There are factors that can modify absorption, such as dietary iron absorption is enhanced by vitamin C and inhibited by phytates, calcium, tannins and certain medications (eg, proton pump inhibitors).
- Promote iron-rich balanced meals:
- Including lean red meat (up to 3-4 times per week) as part of healthy meals will help with meeting iron intakes. The Australian Dietary Guidelines (ADGs) advise up to 65g per day (a maximum of 455g cooked lean red meat per week).
- Encourage lean red meat alongside seafood, legumes, leafy greens, nuts and fortified cereals.
3. Prioritise High-Risk Groups
- Teenage girls: Consider education on iron needs during menstruation, particularly for athletes.
- Pregnant women: Early screening, dietary counselling, and supplementation.
- Perimenopausal women: Screen for heavy menstrual bleeding.
- Vegetarians/Vegans: Provide practical meal plans to meet iron needs.
- Indigenous women: Support culturally relevant nutrition programs.
4. Consider Supplementation
Key Takeaways for GPs
- Iron deficiency is common and often underdiagnosed in Australian women.
- Blood loss and low dietary intake of iron are major contributors.
- Screening, education, and tailored interventions can significantly improve iron status.
- Collaboration with dietitians enhances patient outcomes.
Monique Cashion, is an Accredited Practising Dietitian and Group Manager, Food & Nutrition, Meat & Livestock Australia. This article was commissioned by Meat & Livestock Australia.
The statements or opinions expressed in this article reflect the views of the authors and do not necessarily represent the official policy of the AMA, the MJA or InSight+ unless so stated.
Subscribe to the free InSight+ weekly newsletter here. It is available to all readers, not just registered medical practitioners.
If you would like to submit an article for consideration, send a Word version to mjainsight-editor@ampco.com.au.